Global DCIS, LCIS, Invasive Breast Cancer

2020: A Statistical and Medical Analysis into the Global Incidence and Mortality Rates of DCIS, LCIS, and Invasive (Metastatic) Breast Cancer
Anuragh Sriram and Dr. Lopamudra Das Roy
Published 2020
@BreastCancerHub, All Rights Reserved
Abstract:
Breast cancer is the most common cancer in women worldwide and the second most common cancer overall (1). In 2018, there were over 2 million new cases and over 620 thousand deaths (1). In fact, almost 50% of breast cancer cases and 58% of breast cancer deaths occur in less developed countries (1). Everyday, medical advancements for breast cancer are being made and we are learning so much more about this disease. Yet, how is it that when we possess this wealth of knowledge on the biology/genetics, early-detection, and treatment of breast cancer, incidence rates are continuously on the rise. As mentioned earlier, over half of the breast cancer deaths occur in less developed regions. This is because there is a lack of proper healthcare, education, and outreach in these regions. It is very easy to go to developed and literate parts of the world and educate the population on breast cancer detection and treatment, but it takes more effort to do the same in underdeveloped, illiterate parts of the world. These places are left out and lack access to modern healthcare and medicine and in these regions, the stigma around having breast cancer is still very much at large. This paper examines research studies on the incidence and mortality of DCIS, LCIS, and other invasive breast cancers. The paper also cites statistics from reports put out by the World Health Organization, the American Cancer Society, and the US National Library of Medicine within the last two years. The paper portrays these statistics in the form of graphs, and then offer detailed explanations as to why we are seeing the trends displayed. Extensive research and data collection were performed, with data being collected from health ministries of developing regions like Eastern Asia, Sub-Saharan Africa, South America and were incorporated into our data analysis. This paper was formulated by utilizing research and data from all of these organizations and research studies.
General Breast Cancer Statistics:
The majority of breast cancers are carcinomas of the epithelial cells lining the breast ducts. The graph below shows the total number of female cases and deaths for breast cancer globally. You would have noticed that the data below does not reflect the number of new breast cancer cases and deaths for males in 2018. This is because not much research is done on male breast cancer cases. Quite simply, more research needs to be done into male breast cancer cases.
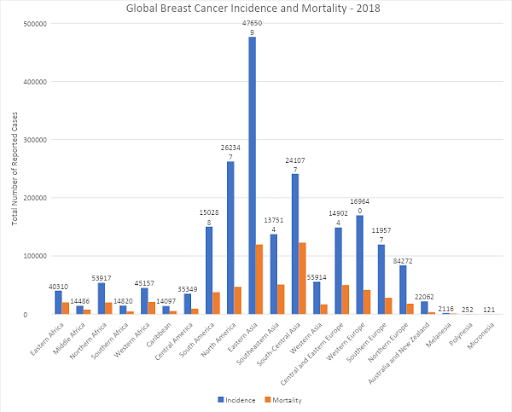
Data Source: Globocan 2018 Breast Cancer Report
Graph Created By: Anuragh Sriram ©Breast Cancer Hub
In Situ Breast Cancers:
The two main types of in situ breast cancer are ductal carcinoma in situ (DCIS) and lobular carcinoma in situ (LCIS).
Ductal Carcinoma in Situ:
DCIS constitutes about 83% of all in situ cases and about 20-25% of all breast cancer cases. It also comprises 17-34% of all mammography detected cases (2).
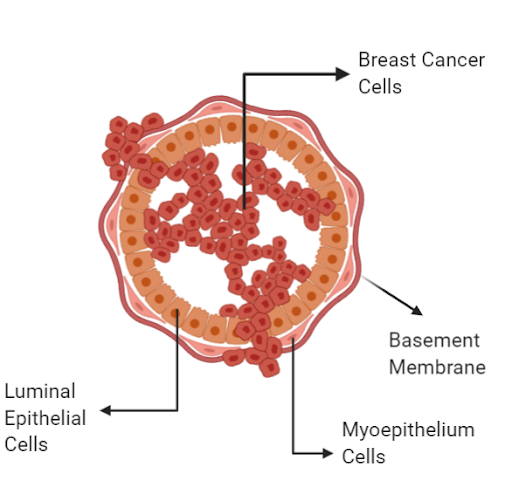
In DCIS, cancer cells replace normal epithelial cells that line the breast ducts, and this may cause the ducts and lobules to expand, as seen in the diagram below. DCIS is considered as a possible precursor to invasive breast cancer. Women with DCIS are ten times more likely to be diagnosed with an invasive breast cancer than women without DCIS. About 40% of DCIS cases progress to invasive cancer (2).

Created by Anurag Sriram @BreastCancerHub, All Rights Reserved
Older age is one of the leading risk factors for being diagnosed with DCIS, as shown in the graph below. During 2016-2018, the median age of DCIS diagnosis in the United States was 62. In addition, DCIS incidence rates in the US during this same time frame were highest among non-Hispanic whites, but mortality rates were highest among non-Hispanic blacks (2).

Lobular Carcinoma in situ:
LCIS constitutes 13% of in situ cases and is less common than DCIS. This condition refers to cancer cells growing within and expanding some of the lobules (milk glands) of the breast. LCIS is widely thought to be a strong risk factor for developing invasive cancer. Women with LCIS are 7-12 times more likely to develop invasive breast cancer than women without LCIS. Like DCIS, old age is a factor in diagnosis of LCIS. In 2019, the median age at diagnosis of LCIS was between 49-50 years, as shown in the graph below. The graph below shows data that extends up to 2011. Although this data is not current, we hope to use this graph to show a general trend in how older age tends to increase the incidence rates of LCIS. No recent data was found on incidence rates of LCIS.

In-situ breast cancer – Developing World Statistics:
In several developing countries, breast cancer incidence rates are increasing dramatically due to changes in reproductive factors and lifestyles (Annals of Oncology, 2018). Over 60% of in situ breast cancer cases occur in the developing world.
While continuing to allow LMIC (Low middle-income countries) access to advanced detection technologies, achieving higher survival and lower incidence rates can be achieved through increased awareness of breast cancer and by developing an excellent and modern primary healthcare system without economic or cultural barriers and which consists of the latest surgical and hormonal treatment.

Data Source: Silverman, B. G. (2017). Survey of Breast Cancer Incidence in the Middle East and the United States. International Journal of Women's Health and Wellness, 3(1). doi:10.23937/2474-1353/1510045
Graph Created By: Anuragh Sriram ©Breast Cancer Hub
Note: The South Africa percentage includes the combined areas of Cape Town, Port Elizabeth, Johannesburg, and East London. This explains its high percentage.
The graph above shows the percentage of all breast cancer cases that were in-situ for various developing regions around the globe. The reasons why these regions in specific were chosen is because these areas have hosted various clinical breast cancer research studies in which data was available.
If we look at Mumbai and Trivandrum, India, we see that they have reported the lowest percentage of in-situ breast cancer cases for the 2017 fiscal year, 8 and 4 percent respectively. At first, one might assume that there was a significant reporting error for these statistics, but if you think about it, it makes sense. Since the percentage was so small, that means that not many people are reporting in-situ breast cancers. DCIS and LCIS constitute Stage 0 breast cancer, which means that the tumor has not metastasized to other body structures yet. The tumor is highly localized and contained within the ducts and lobules of the breast tissue. Thus, a lot of women in these areas would not tend to report this as they do not feel it is serious enough. Due to the lack of early-detection programs and education, a lot of women are letting these tumors grow unchecked, and thus allowing the tumor to progress to an invasive, Stage IV breast cancer. This causes the percentage of reported invasive breast cancer cases to be significantly higher, because the women are only seeking treatment and reporting their conditions once a prominent lump on the breast tissue has been felt.
One explanation for why South Africa retains the highest percentage of reported in-situ breast cancer cases is because it is the most urbanized country in Africa. As such, it is able to offer education to all groups of people, rich and poor. In fact, according to the Cancer Association of South Africa, recent education and outreach programs in small townships such as Soweto have led to more reported cases, which has decreased the incidence rate of invasive breast cancer in the country.
In terms of national cancer planning, countries around the globe require a significant knowledge of the disease burden in the country, which allows doctors to make accurate cancer diagnosis and prognoses. Accurate diagnosis depends on timing and sufficient pathology support. As seen in the graph, various regions of Sub-Saharan and northern Africa have extremely high incidence percentages for in-situ breast cancer because they lack the proper pathology services. Ratios vary from that in Mauritius, where there is approximately 1 pathologist for every 84,133 persons, to Niger where there is one pathologist to 9,264,500 persons (3). Due to the significant lack of pathological services, several citizens in these regions lack the necessary access to mammograms, chemo and endocrine therapy, and surgery, all of which can detect and prevent metastasis of the carcinoma in-situ. Obtaining a complete histopathological review of a breast tissue sample is a challenge in LMIC’s because of the lack of access to high-quality tissue processing facilities and prognostic marker evaluation.
Invasive/Infiltrating Breast Cancer:
About 81% of all breast cancer cases worldwide are invasive (2), which means that the cancer cells have broken through the walls of the glands or ducts where they originated and have now grown into the surrounding breast tissue, as shown in the diagram below.
Trends in Incidence Rates of Invasive Female Breast Cancer:
created by Anurag Sriram, @BreastCancerHub, All rights reserved

In the United States in 2019, an estimated 268,600 new cases of invasive breast cancer were diagnosed among women and approximately 2,670 cases were diagnosed in men. As shown in the graph above, old age is a factor in diagnosis, with the average age of diagnosis in 2019 in the United States being 56 (2).

Data Source: Silverman, B. G. (2017). Survey of Breast Cancer Incidence in the Middle East and the United States. International Journal of Women's Health and Wellness, 3(1). doi:10.23937/2474-1353/1510045
Diagram Created By: Anuragh Sriram ©Breast Cancer Hub
The graph above shows the percentage of all breast cancer cases in developing regions that were reported as invasive. The same developing regions as used in the in-situ graph were used here. When compared to the percentage of in-situ tumors, the incidence of invasive tumors were significantly higher, as expected, with the highest incidence percentages being in Sub-Saharan Africa and Asia. As more individuals start to experience extreme pain in their abdominal region and notice large lumps on their breast tissue, they start reporting their symptoms and start receiving treatment. If more countries were to offer education about early-detection to illiterate and disadvantaged populations, then the problem of high percentages of invasive breast cancer cases can be mitigated to an extent.
What Can Be Done to Improve Breast Cancer Survival in LMIC:
A healthy lifestyle (limiting consumption of alcohol, physical activity, and maintaining healthy body mass indexes) along with avoiding postmenopausal hormonal replacement therapy has the potential to significantly decrease breast cancer incidence rates in LMIC.
Earlier detection, timely surgery, along with education about breast cancer would go a long way in improving survival rates. It is important that citizens of developing world countries become more involved with advocacy of curability and learn more about skilled breast physical examinations. Education efforts need to be direct, and must address the unfortunate reality that many women, especially those with lower income and literacy rates, may not seek medical attention when they feel a breast mass. This could be due to them not knowing what it means or it could also be due to them being concerned about the heavy stigma of having cancer and being potentially ostracized by their community.
In the past, it has been demonstrated that by providing education, more accessible healthcare facilities, trained medical personnel, and effective therapy to disadvantaged populations, people do seek treatment and are profited by it. These efforts were heavily publicized with destigmatizing HIV, HPV, and other diseases. This same doctrine can be applied to breast cancer prevention and treatment in third-world countries.
Providing adequate and affordable access to physical exams and care does not have to be so trivial in nature. Now, several developing areas in Africa and Asia have welcomed international assistance to set up functioning primary care systems that are trusted by communities. One such example is the collaboration between the Ministry of Health in Rwanda, Partners in Health, and the Dana-Farber Cancer Institute in providing remote pathology assessment via telepathology to assist with breast cancer and other pathology diagnoses. The setup of whole slide image scanning and the automation of processing have helped with the provision of timely and complete pathology services for patients with breast cancer in Rwanda. This collaboration has also allowed these disadvantaged communities to gain more access to vital drugs that can be used to treat breast cancer, such as tamoxifen and trastuzumab
References:
https://gco.iarc.fr/today/data/factsheets/cancers/20-Breast-fact-sheet.pdf
Martei YM, Pace LE, Brock JE, Shulman LN. Breast Cancer in Low- and Middle-Income Countries: Why We Need Pathology Capability to Solve This Challenge. Clin Lab Med. 2018;38(1):161-173. doi:10.1016/j.cll.2017.10.013
Shulman, L. N., Willett, W., Sievers, A., & Knaul, F. M. (2010). Breast cancer in developing countries: opportunities for improved survival. Journal of oncology, 2010, 595167. https://doi.org/10.1155/2010/595167
Fleming K. (2019). Pathology and cancer in Africa. Ecancermedicalscience, 13, 945. https://doi.org/10.3332/ecancer.2019.945